
U.S. employers spend over $8,000 per employee annually on health benefits, yet preventable diseases and fragmented care systems waste billions every year. Most companies have no idea where their money actually goes or how to reclaim it.
At The Pledge, we’ve analyzed what separates employers achieving real employer health cost savings from those stuck in the status quo. This guide shows you the concrete strategies, real ROI numbers, and metrics that matter.
Where Healthcare Dollars Actually Disappear
Chronic Disease Drives the Majority of Spending
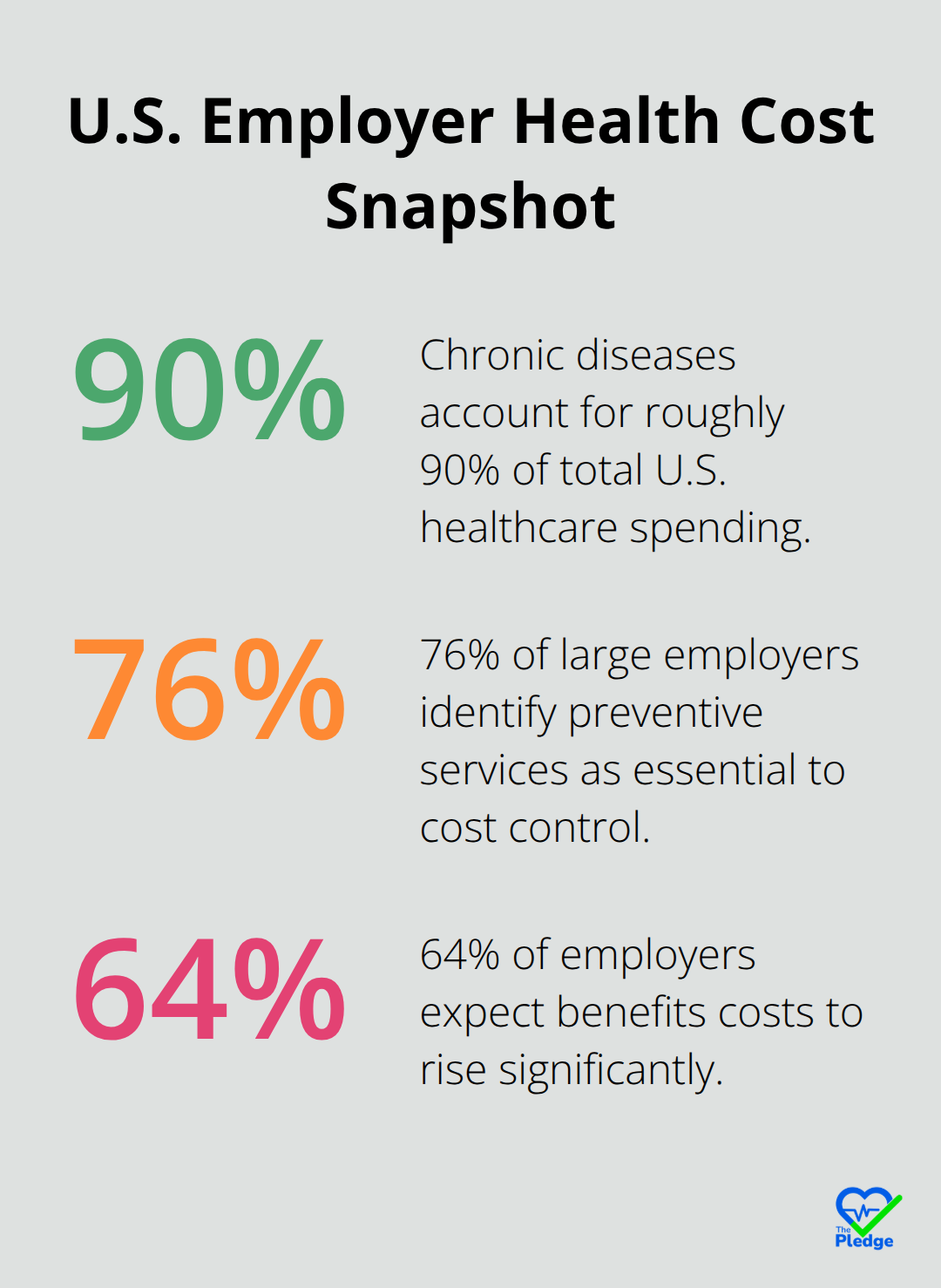
Chronic diseases consume roughly 90% of the United States’ $4.9 trillion annual healthcare spending, according to CDC findings. Yet most employers treat these costs as inevitable overhead rather than a problem with clear solutions. The reality is far different. Employers lose money because preventable conditions like diabetes, hypertension, and cardiovascular disease go undetected until they become emergencies. A worker with uncontrolled diabetes might accumulate thousands in ER visits and hospitalizations when a $200 biometric screening and basic coaching could have prevented the crisis entirely. The Kaiser Family Foundation reports that the average family premium reached nearly $27,000 annually in 2025, with workers contributing about $6,850.
That staggering cost persists partly because employers lack visibility into what drives their claims.
Preventable Admissions Represent Massive Waste
Preventable hospital admissions represent hundreds of thousands in avoidable spending per case. Labcorp’s analysis showed that 76% of large employers identify preventive services as essential to cost control, yet most programs remain fragmented and poorly coordinated, leaving gaps that allow preventable disease to flourish. Early detection and intervention cost far less than emergency treatment, yet employers continue to pay for crises that better systems could have prevented.
Fragmented Systems Create Duplicate Costs
Fragmented care systems compound the waste dramatically. When employees see multiple providers without shared records, duplicate testing becomes routine. A worker might undergo the same imaging study twice because results never reached the next specialist. Pharmacy systems don’t communicate with primary care, so patients take conflicting medications or miss dangerous interactions. Employers paying claims have no way to connect these inefficiencies to their bottom line because data lives in isolated silos.
Poor Engagement Leaves Prevention Opportunities Unused
Poor employee engagement ensures preventive care opportunities slip away entirely. The Labcorp Designing for Impact survey found that 64% of employers expect benefits costs to rise significantly, yet only a fraction actively track whether employees actually use preventive screenings. Without centralized data and proactive outreach, employees miss early detection windows, and employers miss the chance to intervene before minor issues become major expenses. This gap between available coverage and actual utilization represents pure waste-employers pay for benefits employees never access.
Moving From Passive Coverage to Active Coordination
The solution requires moving beyond passive coverage to active coordination, where employers can see the full picture of their workforce’s health, identify high-risk individuals, and connect them to care before minor issues become major expenses. Centralizing health data transforms employers from passive payers into active managers of their healthcare spend. This shift unlocks the ability to track outcomes, measure what works, and redirect dollars toward interventions that actually prevent disease rather than simply treating it after the fact.
How to Build a Healthcare System That Actually Works
Centralize Your Health Data to See What’s Really Happening
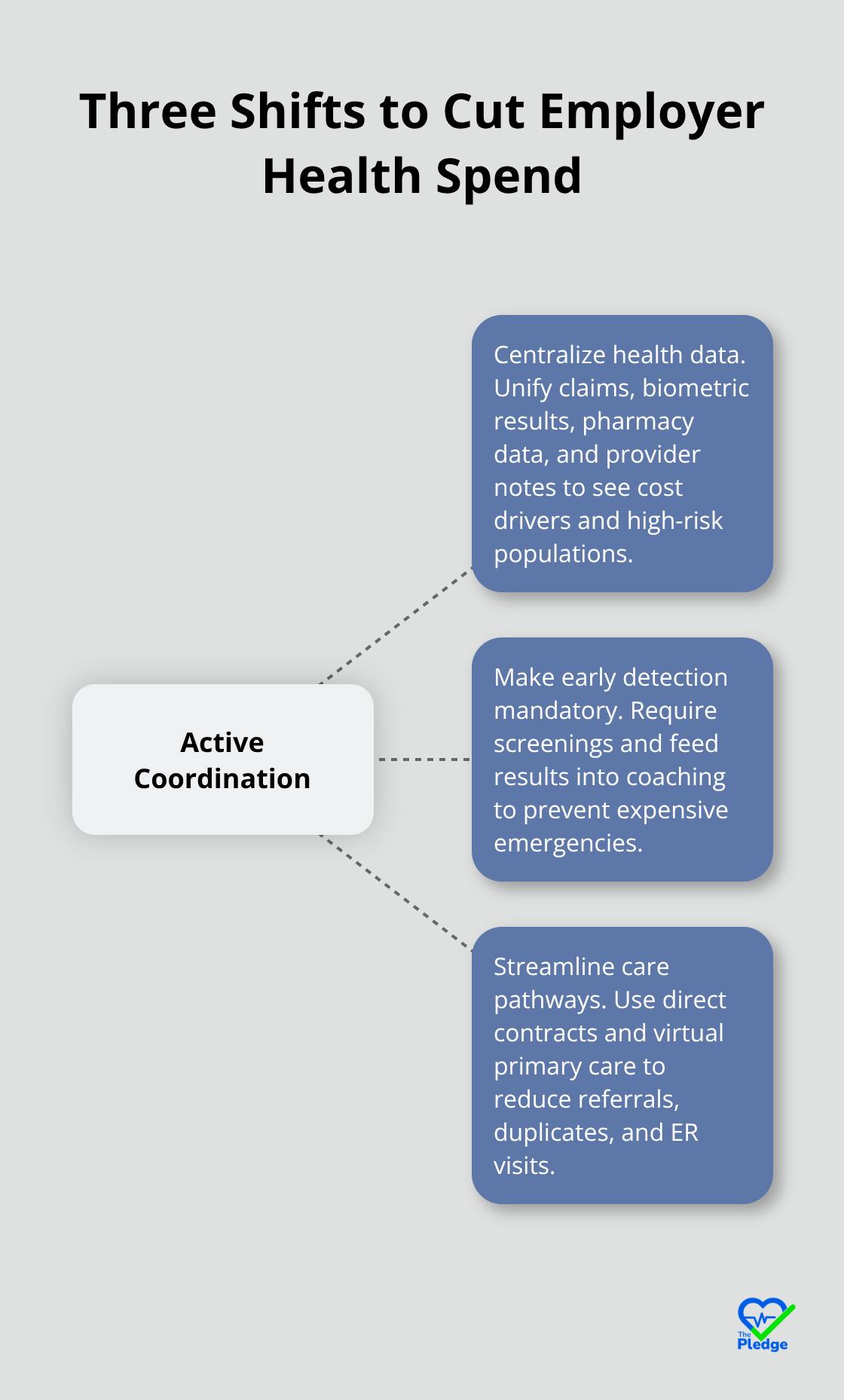
Passive health benefits don’t reduce costs. You need active systems that connect data, identify risk, and coordinate care before problems explode into expensive emergencies. The difference between employers cutting healthcare spending by 15–30% and those stuck paying full freight comes down to three operational shifts that most companies haven’t made yet.
Start by centralizing your health data so you can actually see what’s happening in your workforce. Right now, your claims data lives in one system, your benefits enrollment in another, and provider records scatter across multiple health systems. This fragmentation means you’re flying blind. Comprehensive data analytics can help employers identify cost drivers and implement strategies to mitigate rising healthcare expenses. When you unify this information-claims, biometric results, pharmacy data, provider notes-you gain the visibility to identify your top cost drivers. A tech startup in Austin that switched to a centralized benefits approach reduced per-employee monthly costs from $500 to $300 by aligning coverage with actual workforce needs. The key is moving from abstract premium numbers to concrete insights: Which employees have uncontrolled diabetes? Who’s overdue for cancer screening? Which providers deliver better outcomes at lower cost?
Once you answer these questions with real data, you can act. Kampgrounds Enterprises achieved a 30% reduction in healthcare costs after implementing centralized data management paired with tailored benefits, because they finally knew what they were paying for and why.
Make Early Detection Non-Negotiable, Not Optional
The second shift requires you to make early detection non-negotiable, not optional. Biometric screenings, health risk assessments, and coaching programs only work if participation is high and results feed into coordinated care. Early detection and biometric screening participation rates have grown significantly among large firms offering health benefits. That matters because lowering blood pressure from 125/80 to 110/70 reduces risk of heart attack, stroke, and kidney disease, cutting off the expensive complications that drive your claims. The actionable step here is bundling screening with accountability: don’t just offer biometric testing; require it as part of enrollment, provide immediate feedback, and follow up with targeted coaching for high-risk individuals. Use HSAs or FSAs to incentivize participation-employees who engage in preventive services can earn HSA contributions or premium discounts. This transforms prevention from a nice-to-have into a core operating model. Large employers increasingly use this approach: 60–69% of the largest firms offer incentives tied to health risk assessments and biometric outcomes, driving participation rates that actually move the needle on claims.
Streamline Care Coordination Through Direct Provider Pathways
Third, streamline care coordination by building direct pathways to providers and eliminating waste in the system. Traditional insurance networks are bloated-employees navigate through multiple referrals, duplicate tests, and disconnected specialists. Instead, establish direct contracts with primary care providers, centers of excellence for complex conditions, and virtual-first care options. 30% of firms with 50+ workers now contract directly for virtual primary care, and 45% of those with 1,000+ workers do the same. This matters because virtual primary care is cheaper, faster, and reduces unnecessary emergency room visits. Hotel Pommier used care coordination to reduce absenteeism and boost productivity while cutting costs, proving that when employees can access care easily, outcomes improve. Big Brothers Big Sisters of McHenry County leveraged coordinated benefits with rollover options for unused funds, improving both retention and long-term financial security.
Audit Your Network and Track What Works
The practical step is auditing your current network: Are employees bouncing between providers without shared records? Are specialists ordering tests that primary care already completed? Are your highest-cost employees (those with chronic conditions) receiving proactive management or reactive emergency care? Once you identify these gaps, negotiate narrow networks or direct contracts with providers who commit to coordination and outcome tracking. Track utilization shifts-if virtual primary care visits increase while ER visits drop, you’ve found a lever that works. Data-driven decision making means using your health analytics to target the specific cost drivers in your workforce, whether that’s cardiometabolic disease, pregnancy complications, or oncology, then measuring ROI proxies like risk migration and reduced emergency visits. These three shifts-centralizing data, making prevention mandatory, and streamlining care pathways-create the foundation for measurable cost reduction. The next step is understanding exactly what ROI numbers you should expect from these changes and how to track them.
What ROI Should You Actually Expect
Medical Claims Reduction From Engaged Employees
Vitality’s 2024 survey found that employees engaged in wellbeing programs generate an average of $462 in annual medical claims cost savings per person. That number matters because it’s concrete and repeatable across different employer sizes and industries. When you centralize health data and implement coordinated care, you activate a mechanism that consistently reduces claims. The math is straightforward: if your company has 500 employees and 60% engage in preventive programs, you’re looking at roughly $138,600 in annual medical claims reduction from that cohort alone. Labcorp’s biometric screening program combined with health coaching showed 31% of participants improved their blood pressure risk level within two years. That shift from elevated to normal blood pressure reduces downstream claims for heart attack, stroke, and kidney disease by thousands per case.
Productivity Gains and Turnover Reduction Dwarf Claims Savings
Add productivity gains and turnover reduction to the equation, and the number climbs significantly. Deloitte data shows absenteeism costs about $3,600 per hourly employee and $2,650 per salaried employee annually. McKinsey research indicates employees with mental-health and well-being challenges are 4 times more likely to leave their employer. These aren’t abstract figures-they’re direct hits to your payroll and turnover costs. Companies prioritizing wellbeing achieve up to 20% higher productivity. That translates to concrete output gains-fewer errors, faster project completion, better customer interactions. Track turnover specifically among employees engaged in wellness programs versus those who aren’t; the retention difference often exceeds 15%, and retention savings dwarf medical claims savings for most employers.
Calculate Your Actual ROI With Real Numbers
Real ROI calculation works like this: if you invest $100,000 annually in centralized data infrastructure, screening programs, and care coordination, and generate $150,000 in medical claims reduction plus $80,000 in productivity gains and reduced turnover costs, your ROI is 230%. The formula is straightforward: (Savings – Costs) / Costs. Most employers underestimate the productivity and retention components because they’re harder to quantify, but they’re often larger than the claims savings alone. Companies that bundle preventive screening with care coordination see risk migration happen fast. When you implement direct primary care contracts or virtual-first care options, measure how quickly ER visits drop-that’s your immediate cost signal.
Track Metrics That Actually Drive ROI
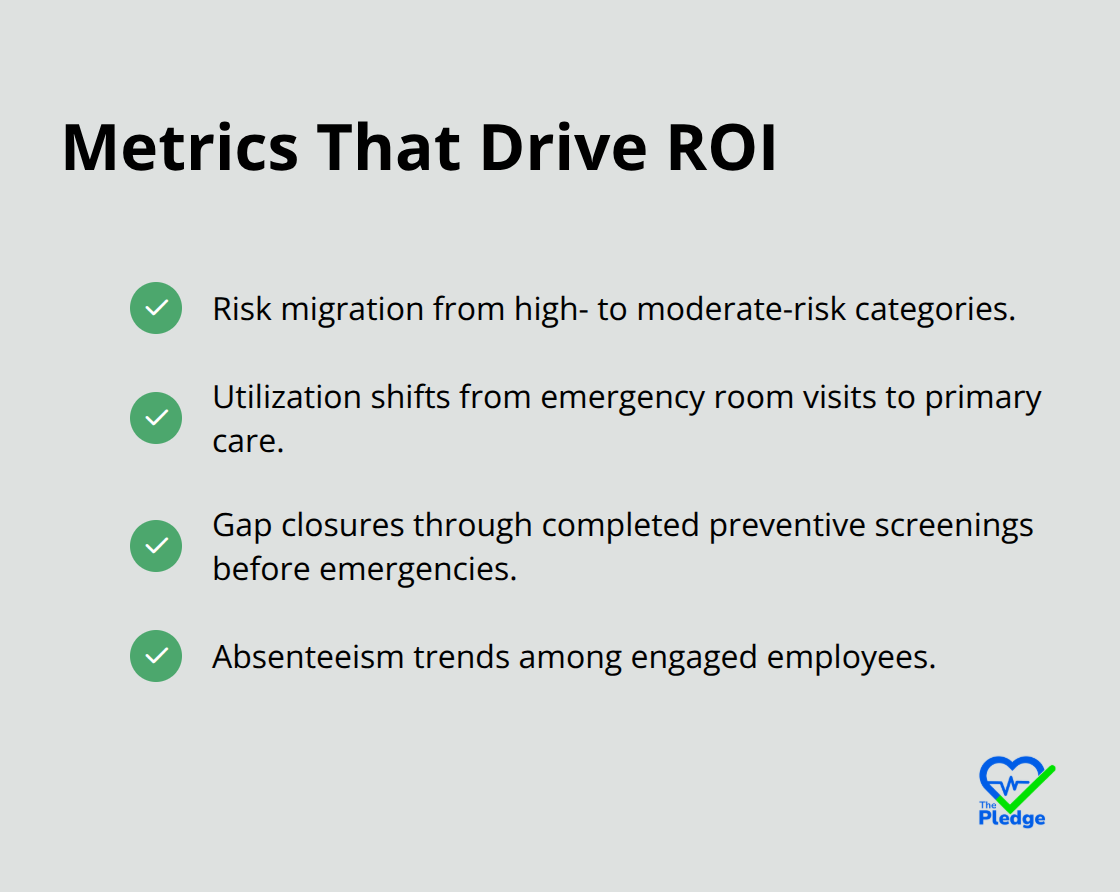
The critical move is tracking the right metrics throughout the year, not waiting for annual renewal to measure impact. Participation rates in health risk assessments and biometric screenings matter, but the metrics that actually drive ROI are risk migration (how many employees move from high-risk to moderate-risk categories), utilization shifts (emergency room visits declining while primary care visits increase), gap closures (preventive screenings completed before they become emergencies), and absenteeism trends.
Track whether employees with chronic conditions shift from reactive emergency care to proactive management; that shift cuts thousands per employee per year. When you measure these metrics monthly, you can adjust quickly if participation lags or if certain provider partnerships underperform. This visibility allows you to reallocate resources toward what actually works in your specific workforce rather than running generic programs that might miss your actual cost drivers.
Build Systems That Sustain ROI Over Time
Real ROI emerges over 18–24 months as preventive care catches conditions early, care coordination eliminates redundant testing, and engaged employees stay longer. Treat wellness as a system, not a line item. Most companies launch a program, measure participation for a quarter, and move on. Instead, build a dashboard that tracks these metrics monthly so you can see exactly which interventions move the needle in your workforce. The mistake most companies make is running generic programs that might miss your actual cost drivers. Data-driven decision making means using your health analytics to target the specific cost drivers in your workforce-whether that’s cardiometabolic disease, pregnancy complications, or oncology-then measuring ROI proxies like risk migration and reduced emergency visits.
Final Thoughts
Employer health cost savings emerge from three operational shifts that separate high performers from the rest. You must centralize your health data to see what actually happens in your workforce, make early detection mandatory through screenings and coaching, and streamline care coordination by building direct pathways to providers. These concrete actions generate the 15–30% spending reductions that most employers never achieve because they treat healthcare as a fixed cost rather than a system they can optimize.
The metrics that matter most reveal where your money actually goes and what interventions work. Track risk migration to show how many employees move from high-risk to moderate-risk categories, measure utilization shifts as emergency room visits decline and primary care visits increase, monitor gap closures where preventive screenings catch conditions before they become emergencies, and watch absenteeism trends among engaged employees. When you measure these metrics monthly, you adjust quickly if something underperforms and reallocate resources toward what actually works in your specific workforce. Real ROI emerges over 18–24 months as preventive care catches conditions early, care coordination eliminates redundant testing, and engaged employees stay longer-the math typically generates 200–300% ROI when you account for medical claims reduction ($462 per engaged employee annually), productivity gains (up to 20%), and turnover savings that often exceed claims savings.
Start now by auditing your current network to identify gaps where employees bounce between providers without shared records, then centralize your health data immediately by integrating claims, biometric results, pharmacy data, and provider notes into one system. Implement direct primary care contracts or virtual-first care options to reduce unnecessary emergency room visits, and build a dashboard that tracks your key metrics monthly rather than waiting for annual renewal to measure impact. We at The Pledge built a platform specifically designed to centralize health data and drive the engagement that transforms these strategies into measurable results-explore how The Pledge can accelerate your employer health cost savings and help you achieve the ROI numbers outlined in this guide.
![[Guide] Incentives That Drive Preventive Health Participation](https://thepledge.app/wp-content/uploads/emplibot/Guide_-Incentives-That-Drive-Preventive-Health-Participation_1783650286-300x168.jpeg)





